
Supplying power to bioelectronic implants is essential for long-term operations. However, placing a socket on them can invite invasions from microbial intruders, and wireless charging antennas are often bulky. Now scientists have created a new implantable power outlet accessible via needle they say can overcome the challenges faced by previous charging techniques.
“It is intended to serve as a general access point that could be integrated with many existing implantable bioelectronic devices, including sensors, neural interfaces, stimulators, and battery-powered systems,” says Dion Khodagholy, an associate professor of electrical engineering and computer science at the University of California, Irvine.
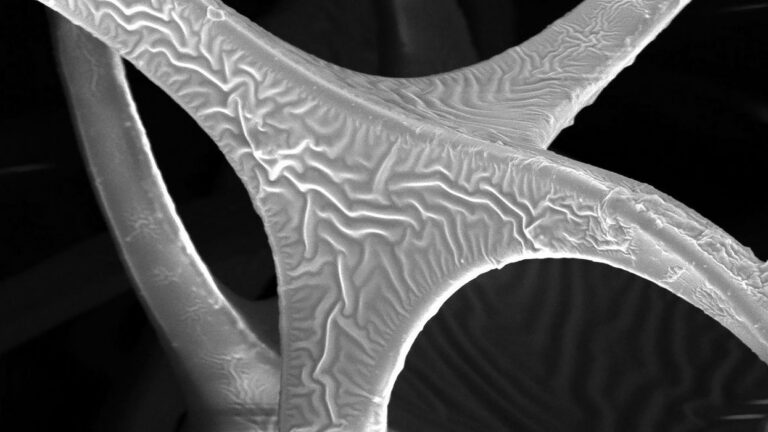
The new device, which the researchers call an implantable bioelectric outlet, is made mostly of a soft spongy plastic with pores about 150 micrometers wide, comparable to a very fine needle’s diameter. They first dipped the sponge in a highly electrically conductive polymer to coat its pores with a layer of the polymer 100 to 200 nanometers thick. Next, they dipped the sponge in a silicone rubber solution to provide a protective electrically insulating jacket around its exterior. Finally, they sandwiched several of these jacketed sponge layers between unmodified layers of the sponge and covered the entire stack with silicone rubber to form a module useful for applications.
“With our approach, the device remains completely under the skin,” says Hyung Joon Shim, a postdoctoral scholar in electrical engineering at UC Irvine. “A needle is inserted only when electrical access is needed and is removed afterward.”
Implant Charging With a Jab
In experiments on mice and rats, the scientists coupled their outlets with implants such as neural interface devices. By inserting a needle into the outlets, the researchers could recharge the batteries of the neural interface devices as well as receive data from them at the implants’ maximum transfer speeds of nearly 16 megabits per second. They detailed their findings 8 July in the journal Science Advances.
In addition, in experiments on pigs, the researchers combined their outlets with implants capable of delivering electrical stimulation, which previous work found could help boost nerve healing. The scientists could deliver 20-microampere electric pulses, each lasting 100 milliseconds, for an extended period using the outlet to help keep the electrical stimulation going.
The porous, resilient nature of the device prevented cracks and tears from growing and spreading when the device was poked with a needle, even with repeated jabs with needles ranging from 30 gauge (0.1 millimeter wide) to 18 gauge (1.5 mm wide). “In our laboratory tests, the device maintained its electrical performance and insulation after more than 100 insertions,” Khodagholy says. In addition, the outlet’s jacketed layers are electrically conductive throughout, so a needle “does not need to hit one very small point to make a connection.”
The scientists had their outlets implanted in mice for more than a year. The outlets did not degrade during that time, nor did they cause any visible problems for the rodents. “Long-term safety and stability are among the most important requirements for any implantable technology,” says Jennifer Gelinas, an associate professor of pediatrics and anatomy and neurobiology at UC Irvine.
Refining the Outlet for Real-World Use
In the experiments, the animals were anesthetized, which helped keep the charging needles stable. “For use in an awake subject, the needle and attached wire could be secured to the skin with medical tape or an adhesive dressing, similar to an IV needle, to prevent movement during charging or data transfer,” Gelinas says.
Passing a needle through the skin to connect with the outlet “would probably cause some brief discomfort, similar to an injection or a small IV needle,” Gelinas notes. “Future versions could use smaller needles, topical anesthetics, or coatings that reduce pain and inflammation.”
In addition, “the implantable bioelectric outlet probe would not need a hollow channel for delivering fluid, which means that a dedicated implantable bioelectric outlet needle probe could potentially be made even thinner than a conventional injection needle,” Gelinas explains. “That may further reduce pain and irritation.”
The researchers note that their outlet could be used together with wireless technology. “For example, an implant might use wireless communication for routine operation, and use the implantable bioelectronic outlet only when direct access is more useful, such as for fast charging, downloading large amounts of data, updating the device, or performing maintenance,” Shim says.
The researchers fabricated the outlet “relatively easily using readily available materials,” Shim adds. “That could make future manufacturing and translation more practical.”
The scientists caution that their device is not yet ready for use in patients. “We would need to evaluate pain, skin irritation, infection risk, tissue response, and whether the electrical performance changes after many access sessions,” Gelinas says.













 A volunteer clad in the new exoskeleton wears sensors to monitor metabolism while walking on a treadmill.Ziqi Zhang, Wei Yu, et al.
A volunteer clad in the new exoskeleton wears sensors to monitor metabolism while walking on a treadmill.Ziqi Zhang, Wei Yu, et al.














