
Inside a cavernous hall at the Swiss-French border, the air hums with high voltage and possibility. From his perch on the wraparound observation deck, physicist Walter Wuensch surveys a multimillion-dollar array of accelerating cavities, klystrons, modulators, and pulse compressors—hardware being readied to drive a new generation of linear particle accelerators.
Wuensch has spent decades working with these machines to crack the deepest mysteries of the universe. Now he and his colleagues are aiming at a new target: cancer. Here at CERN (the European Organization for Nuclear Research) and other particle-physics labs, scientists and engineers are applying the tools of fundamental physics to develop a technique called FLASH radiotherapy that offers a radical and counterintuitive vision for treating the disease.
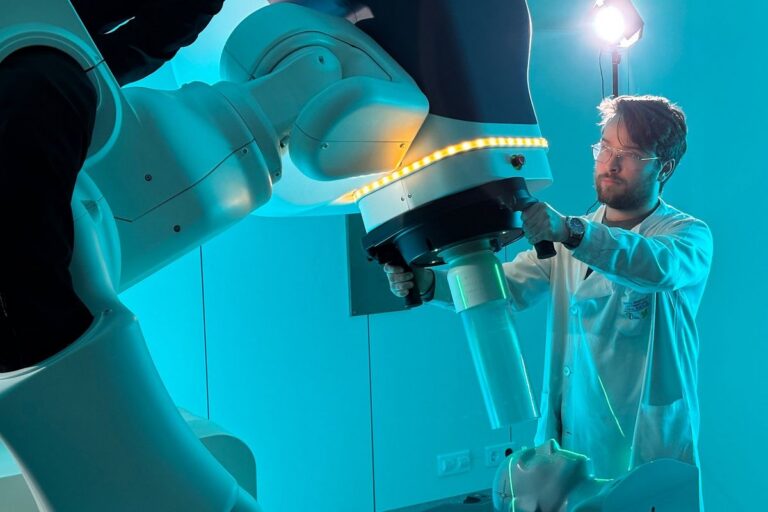
 CERN researcher Walter Wuensch says the particle physics lab’s work on FLASH radiotherapy is “generating a lot of excitement.”CERN
CERN researcher Walter Wuensch says the particle physics lab’s work on FLASH radiotherapy is “generating a lot of excitement.”CERN
Radiation therapy has been a cornerstone of cancer treatment since shortly after Wilhelm Conrad Röntgen discovered X-rays in 1895. Today, more than half of all cancer patients receive it as part of their care, typically in relatively low doses of X-rays delivered over dozens of sessions. Although this approach often kills the tumor, it also wreaks havoc on nearby healthy tissue. Even with modern precision targeting, the potential for collateral damage limits how much radiation doctors can safely deliver.
FLASH radiotherapy flips the conventional approach on its head, delivering a single dose of ultrahigh-power radiation in a burst that typically lasts less than one-tenth of a second. In study after study, this technique causes significantly less injury to normal tissue than conventional radiation does, without compromising its antitumor effect.
At CERN, which I visited last July, the approach is being tested and refined on accelerators that were never intended for medicine. If ongoing experiments here and around the world continue to bear out results, FLASH could transform radiotherapy—delivering stronger treatments, fewer side effects, and broader access to lifesaving care.
“It’s generating a lot of excitement,” says Wuensch, a researcher at CERN’s Linear Electron Accelerator for Research (CLEAR) facility. “We accelerator people are thinking, Oh, wow, here’s an application of our technology that has a societal impact which is more immediate than most high-energy physics.”
The Unlikely Birth of FLASH Therapy
The breakthrough that led to FLASH emerged from a line of experiments that began in the 1990s at Institut Curie in Orsay, near Paris. Researcher Vincent Favaudon was using a low-energy electron accelerator to study radiation chemistry. Targeting the accelerator at mouse lungs, Favaudon expected the radiation to produce scar tissue, or fibrosis. But when he exposed the lungs to ultrafast blasts of radiation, at doses a thousand times as high as what’s used in conventional radiation therapy, the expected fibrosis never appeared.
Puzzled, Favaudon turned to Marie-Catherine Vozenin, a radiation biologist at Curie who specialized in radiation-induced fibrosis. “When I looked at the slides, there was indeed no fibrosis, which was very, very surprising for this type of dose,” recalls Vozenin, who now works at Geneva University Hospitals, in Switzerland.
How to Measure Radiation Doses
Radiation therapy uses a variety of units to refer to the amount of energy received by the patient. Here are the main ones under the International System of Units, or SI.
Gray (Gy): A measure of the absorbed dose—that is, how much radiation energy is absorbed by the body. One gray equals 1 joule of radiation energy per kilogram of matter. FLASH delivers a single dose of 40 Gy or more in a fraction of a second. Conventional radiation therapy, by contrast, may deliver a total dose of 40 to 80 Gy but over the course of several weeks.
Sievert (Sv): A measure of the effective dose—that is, the health effects of the radiation, with different types of ionizing radiation (gamma rays, X-rays, alpha particles, and so on) having different effects. One sievert equals 1 joule per kilogram weighted for the biological effectiveness of the radiation and the tissues exposed.
The pair expanded the experiments to include cancerous tumors. The results upended a long-held trade-off of radiotherapy: the idea that you can’t destroy a tumor without also damaging the host. “This differential effect is really what we want in radiation oncology, not damaging normal tissue but killing the tumors,” Vozenin says.
They repeated the protocol across different types of tissue and tumors. By 2014, they had gathered enough evidence to publish their findings in Science Translational Medicine. Their experiments confirmed that delivering an ultrahigh dose of 10 gray or more in less than a tenth of a second could eradicate tumors in mice while leaving surrounding healthy tissue virtually unharmed. For comparison, a typical chest X-ray delivers about 0.1 milligray, while a session of conventional radiation therapy might deliver a total of about 2 gray per day. (The authors called the effect “FLASH” because of the quick, high doses involved, but it’s not an acronym.)

Many cancer experts were skeptical. The FLASH effect seemed almost too good to be true. “It didn’t get a lot of traction at first,” recalls Billy Loo, a Stanford radiation oncologist specializing in lung cancer. “They described a phenomenon that ran counter to decades of established radiobiology dogma.”
But in the years since then, researchers have observed the effect across a wide range of tumor types and animals—beyond mice to zebra fish, fruit flies, and even a few human subjects, with the same protective effect in the brain, lungs, skin, muscle, heart, and bone.
Why this happens remains a mystery. “We have investigated a lot of hypotheses, and all of them have been wrong,” says Vozenin. Currently, the most plausible theory emerging from her team’s research points to metabolism: Healthy and cancerous cells may process reactive oxygen species—unstable oxygen-containing molecules generated during radiation—in very different ways.
Adapting Accelerators for FLASH
At the time of the first FLASH publication, Loo and his team at Stanford were also focused on dramatically speeding up radiation delivery. But Loo wasn’t chasing a radiobiological breakthrough. He was trying to solve a different problem: motion.
“The tumors that we treat are always moving targets,” he says. “That’s particularly true in the lung, where because of breathing motion, the tumors are constantly moving.”
To bring FLASH therapy out of the lab and into clinical use, researchers like Vozenin and Loo needed machines capable of delivering fast, high doses with pinpoint precision deep inside the body. Most early studies relied on low-energy electron beams like Favaudon’s 4.5-megaelectron-volt Kinetron—sufficient for surface tumors, but unable to reach more than a few centimeters into a human body. Treating deep-seated cancers in the lung, brain, or abdomen would require far higher particle energies.

They also needed an alternative to conventional X-rays. In a clinical linac, X-ray photons are produced by dumping high-energy electrons into a bremsstrahlung target, which is made of a material with a high atomic number, like tungsten or copper. The target slows the electrons, converting their kinetic energy into X-ray photons. It’s an inherently inefficient process that wastes most of the beam power as heat and makes it extremely difficult to reach the ultrahigh dose rates required for FLASH. High-energy electrons, by contrast, can be switched on and off within milliseconds. And because they have a charge and can be steered by magnets, electrons can be precisely guided to reach tumors deep within the body. (Researchers are also investigating protons and carbon ions; see the sidebar, “What’s the Best Particle for FLASH Therapy?”)
Loo turned to the SLAC National Accelerator Laboratory in Menlo Park, Calif., where physicist Sami Gamal-Eldin Tantawi was redefining how electromagnetic waves move through linear accelerators. Tantawi’s findings allowed scientists to precisely control how energy is delivered to particles—paving the way for compact, efficient, and finely tunable machines. It was exactly the kind of technology FLASH therapy would need to target tumors deep inside the body.
Meanwhile, Vozenin and other European researchers turned to CERN, best known for its 27-kilometer Large Hadron Collider (LHC) and the 2012 discovery of the Higgs boson, the “God particle” that gives other particles their mass.
RELATED: AI Hunts for the Next Big Thing in Physics
CERN is also home to a range of smaller linear accelerators—including CLEAR, where Wuensch and his team are adapting high-energy physics tools for medicine.
What’s the Best Particle for FLASH Therapy?
Even as research on FLASH radiotherapy advances, a central question remains: What kind of particle will deliver it best? The main contenders are electrons, protons, and carbon ions. Each has distinct advantages, limitations, and implications for cost, complexity, and clinical reach.
Electrons—long used to treat surface tumors and to generate X-rays—are light, nimble particles, far easier to control than protons or carbon ions. At low energies, they stop quickly in tissue, but new high-energy systems can drive electrons deeper. Now researchers are working on machines that combine multiple high-energy beams at different angles to let doctors sculpt radiation doses that match the tumor’s shape.
That principle underpins Billy Loo’s PHASER (Pluridirectional High-energy Agile Scanning Electron Radiotherapy) system, developed at Stanford and SLAC and licensed to a startup called TibaRay. An array of high-efficiency linacs generates X-ray beams from many directions at once. Their high output overcomes the inefficiency of electron-to-photon conversion to deliver the dose at FLASH speed. Beam convergence at the tumor and electronic shaping conform the dose in three dimensions, producing uniform coverage with relatively simple infrastructure.
Protons have led the way in early clinical trials, largely because existing proton therapy centers can be adapted to deliver FLASH doses. In 2020, the University of Cincinnati Health launched the first human FLASH trial to use proton beams, to treat cancer that had metastasized to bones. “If I want to be pragmatic, the proton beam is ready to go, so let’s move with what we have,” says Geneva University Hospitals’ Marie-Catherine Vozenin.
Protons can penetrate up to 30 centimeters, reaching deep-seated tumors. But the delivery of protons in a continuous beam limits the dose rates. Also, proton systems are far larger and more expensive than, say, X-ray machines, which will likely constrain their availability to specialized centers.
Carbon ions, used in a handful of elite facilities, offer even higher precision and biological effectiveness compared to electrons and protons. Their Bragg peak—a sudden deposition of energy at a specific depth—makes them appealing for deep or complex tumors. But that unmatched precision comes at a steep price, with each facility costing upward of US $300 million. —T.C.
Unlike the LHC, which loops particles around a massive ring to build up energy before smashing them together, linear accelerators like CLEAR send particles along a straight, one-time path. That setup allows for greater precision and compactness, making it ideal for applications like FLASH.
At the heart of the CLEAR facility, Wuensch points out the 200-MeV linear accelerator with its 20-meter beamline. This is “a playground of creativity,” he says, for the physicists and engineers who arrive from all over the world to run experiments.
The process begins when a laser pulse hits a photocathode, releasing a burst of electrons that form the initial beam. These electrons travel through a series of precisely machined copper cavities, where high-frequency microwaves push them forward. The electrons then move through a network of magnets, monitors, and focusing elements that shape and steer them toward the experimental target with submillimeter precision.
Instead of a continuous stream, the electron beam is divided into nanosecond-long bunches—billions of electrons riding the radio-frequency field like surfers. Inside the accelerator’s cavities, the field flips polarity 12 billion times per second, so timing is everything: Only electrons that arrive perfectly in phase with the accelerating wave will gain energy. That process repeats through a chain of cavities, each giving the bunches another push, until the beam reaches its final energy of 200 MeV.

Much of this architecture draws directly from the Compact Linear Collider study, a decades-long CERN project aimed at building a next-generation collider. The proposed CLIC machine would stretch 11 kilometers and collide electrons and positrons at 380 gigaelectron volts. To do that in a linear configuration—without the multiple passes around a ring like the LHC—CERN engineers have had to push for extremely high acceleration gradients to boost the electrons to high energies over relatively short distances—up to 100 megavolts per meter.
Wuensch leads me to a large experimental hall housing prototype structures from the CLIC effort, and points out the microwave devices that now help drive FLASH research. Though the future of CLIC as a collider remains uncertain, its infrastructure is already yielding dividends: smaller, high-gradient accelerators that may one day be as suited for curing cancer as they are for smashing particles.
RELATED: Four Ways Engineers Are Trying to Break Physics
The power behind the high gradients comes from CERN’s Xboxes, the X-band RF systems that dominate the experimental hall. Each Xbox houses a klystron, modulator, pulse compressor, and waveguide network to generate and shape the microwave pulses. The pulse compressors store energy in resonant cavities and then release it in a microsecond burst, producing peaks of up to 200 megawatts; if it were continuous, that’s enough to power at least 40,000 homes. The Xboxes let researchers fine-tune the power, timing, and pulse shape.
According to Wuensch, many of the recent accelerator developments were enabled by advances in computer simulation and high-precision three-dimensional machining. These tools allow the team to iterate quickly, designing new accelerator components and improving beam control with each generation.
Still, real-world challenges remain. The power demands are formidable, as are the space requirements; for all the talk of its “compact” design, the original CLIC was meant to span kilometers. Obviously, a hospital needs something that’s actually compact.
“A big challenge of the project,” says Wuensch, “is to transform this kind of technology and these kinds of components into something that you can imagine installing in a hospital, and it will run every day reliably.”
To that end, CERN researchers have teamed up with the Lausanne University Hospital (known by its French acronym, CHUV) and the French medical technology company Theryq to design a hospital facility capable of treating large and deep-seated tumors with the very short time scales needed for FLASH and scaled down to fit in a clinical setting.
Theryq’s Approach to FLASH
Theryq’s research center and factory are located in southern France, near the base of Montagne Sainte-Victoire, a jagged spine of limestone that Paul Cézanne painted dozens of times, capturing its shifting light and form.
“The solution that we are trying to develop here is something which is extremely versatile,” says Ludovic Le Meunier, CEO of the expanding company. “The ultimate goal is to be able to treat any solid tumor anywhere in the body, which is about 90 percent of the cancer these days.”
 Theryq’s FLASHDEEP system, under development with CERN and the company’s clinical partners, has a 13.5-meter-long, 140-MeV linear accelerator. That’s strong enough to treat tumors at depths of up to about 20 centimeters in the body. The patient will remain in a supported standing position during the split-second irradiation.THERYQ
Theryq’s FLASHDEEP system, under development with CERN and the company’s clinical partners, has a 13.5-meter-long, 140-MeV linear accelerator. That’s strong enough to treat tumors at depths of up to about 20 centimeters in the body. The patient will remain in a supported standing position during the split-second irradiation.THERYQ
Theryq’s push to bring FLASH radiotherapy from the lab to clinic has followed a three-pronged rollout, with each device engineered for a specific depth and clinical use. The first machine, FLASHKNiFE, was unveiled in 2020. Designed for superficial tumors and intraoperative use, the system delivers electron beams at 6 or 9 MeV. A prototype installed that same year at CHUV is conducting a phase-two trial for patients with localized skin cancer.
More recently, Theryq launched FLASHLAB, a compact, 7-MeV platform for radiobiology research.
The company’s most ambitious system, FLASHDEEP, is still under development. The 13.5-meter-long electron source will deliver very high-energy electrons of as much as 140 MeV up to 20 centimeters inside the body in less than 100 milliseconds. An integrated CT scanner, built into a patient-positioning system developed by Leo Cancer Care, captures images that stream directly into the treatment-planning software, enabling precise calculation of the radiation dose. “Before we actually trigger the beam or the treatment, we make stereo images to verify at the very last second that the tumor is exactly where it should be,” says Theryq technical manager Philippe Liger.
FLASH Therapy Moves to Animal Tests
While CERN’s CLEAR accelerator has been instrumental in characterizing FLASH parameters, researchers seeking to study FLASH in living organisms must look elsewhere: CERN doesn’t allow animal experiments on-site. That’s one reason why a growing number of scientists are turning to PITZ, the Photo Injector Test Facility in Zeuthen, a leafy lakeside suburb of Berlin.
PITZ is part of Germany’s national accelerator lab and is responsible for developing the electron source for the European X-ray Free-Electron Laser. Now PITZ is emerging as a hub for FLASH research, with an unusually tunable accelerator and a dedicated biomedical lab to ensure controlled conditions for preclinical studies.

 At Germany’s Photo Injector Test Facility in Zeuthen (PITZ), the electron-beam accelerator [top] is used to irradiate biological targets in early-stage animal tests of FLASH radiotherapy [bottom].Top: Frieder Mueller; Bottom: MWFK
At Germany’s Photo Injector Test Facility in Zeuthen (PITZ), the electron-beam accelerator [top] is used to irradiate biological targets in early-stage animal tests of FLASH radiotherapy [bottom].Top: Frieder Mueller; Bottom: MWFK
“The biggest advantage of our facility is that we can do a very stepwise, very defined and systematic study of dose rates,” says Anna Grebinyk, a biochemist who heads the new biomedical lab, “and systematically optimize the FLASH effect to see where it gets the best properties.”
The experiments begin with zebra-fish embryos, prized for early-stage studies because they’re transparent and develop rapidly. After the embryos, researchers test the most promising parameters in mice. To do that, the PITZ team uses a small-animal radiation research platform, complete with CT imaging and a robotic positioning system adapted from CERN’s CLEAR facility.
What sets PITZ apart is the flexibility of its beamline. The 30-meter accelerator system steers electrons with micrometer precision, producing electron bunches with exceptional brightness and emittance—a metric of beam quality. “We can dial in any distribution of bunches we want,” says Frank Stephan, group leader at PITZ. “That gives us tremendous control over time structure.”
Timing matters. At PITZ, the laser-struck photocathode generates electron bunches that are accelerated immediately, at up to 60 million volts per meter. A fast electromagnetic kicker system acts as a high-speed gatekeeper, selectively deflecting individual electron bunches from a high-repetition beam and steering them according to researchers’ needs. This precise, bunch-by-bunch control is essential for fine-tuning beam properties for FLASH experiments and other radiation therapy studies.
“The idea is to make the complete treatment within one millisecond,” says Stephan. “But of course, you have to [trust] that within this millisecond, everything works fine. There is not a chance to stop [during] this millisecond. It has to work.”
Regulating the dose remains one of the biggest technical hurdles in FLASH. The ionization chambers used in standard radiotherapy can’t respond accurately when dose rates spike hundreds of times higher in a matter of microseconds. So researchers are developing new detector systems to precisely measure these bursts and keep pace with the extreme speed of FLASH delivery.
FLASH as a Research Tool
Beyond its therapeutic potential, FLASH may also open new windows to illuminate cancer biology. “What is really, really superinteresting, in my opinion,” says Vozenin, “is that we can use FLASH as a tool to understand the difference between normal tissue and tumors. There must be something we’re not aware of that really distinguishes the two—and FLASH can help us find it.” Identifying those differences, she says, could lead to entirely new interventions, not just with radiation, but also with drugs.
Vozenin’s team is currently testing a hypothesis involving long-lived proteins present in healthy tissue but absent in tumors. If those proteins prove to be key, she says, “we’re going to find a way to manipulate them—and perhaps reverse the phenomenon, even [turn] a tumor back into a normal tissue.”
Proponents of FLASH believe it could help close the cancer care gap worldwide; in low-income countries, only about 10 percent of patients have access to radiotherapy, and in middle-income countries, only about 60 percent of patients do, according to the International Atomic Energy Agency. Because FLASH treatment can often be delivered in a single brief session, it could spare patients from traveling long distances for weeks of treatment and allow clinics to treat many more people.
High-income countries stand to benefit as well. Fewer sessions mean lower costs, less strain on radiotherapy facilities, and fewer side effects and disruptions for patients.
The big question now is, How long will it take? Researchers I spoke with estimate that FLASH could become a routine clinical option in about 10 years—after the completion of remaining preclinical studies and multiphase human trials, and as machines become more compact, affordable, and efficient. Much of the momentum comes from a growing field of startups competing to build devices, but the broader scientific community remains remarkably open and collaborative.
“Everyone has a relative who knows about cancer because of their own experience,” says Stephan. “My mother died of it. In the end, we want to do something good for mankind. That’s why people work together.”
This article appears in the March 2026 print issue.

























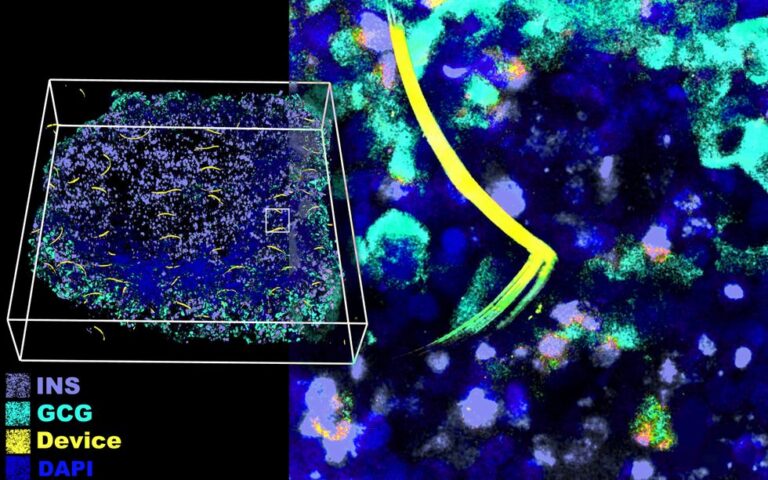

 Passing light through the cyborg organoid while it’s under a microscope shows the flexible electronic device.
Passing light through the cyborg organoid while it’s under a microscope shows the flexible electronic device. 


